The need for mental health support is greater than ever before. Therapists are struggling with all the paperwork; systems that clinics currently use are designed for primary care, not for therapy; some people can’t get an appointment to see a mental health professional for months.
These are all because of the urgent need for better Behavioral Health Software Development solutions in the healthcare technology industry.
If you are a healthcare organization that’s considering going digital, or if you’re a software developer building behavioral health software solutions, then this guide presents exactly what you need to know about building these types of solutions. No fluff; no 15-step frameworks; just a straightforward outline of what to build, how much it costs, and why most projects fail when it comes to behavioral health software development.
What is Behavioral Health Software?
But before we get into anything else, let’s straighten out the confusion.
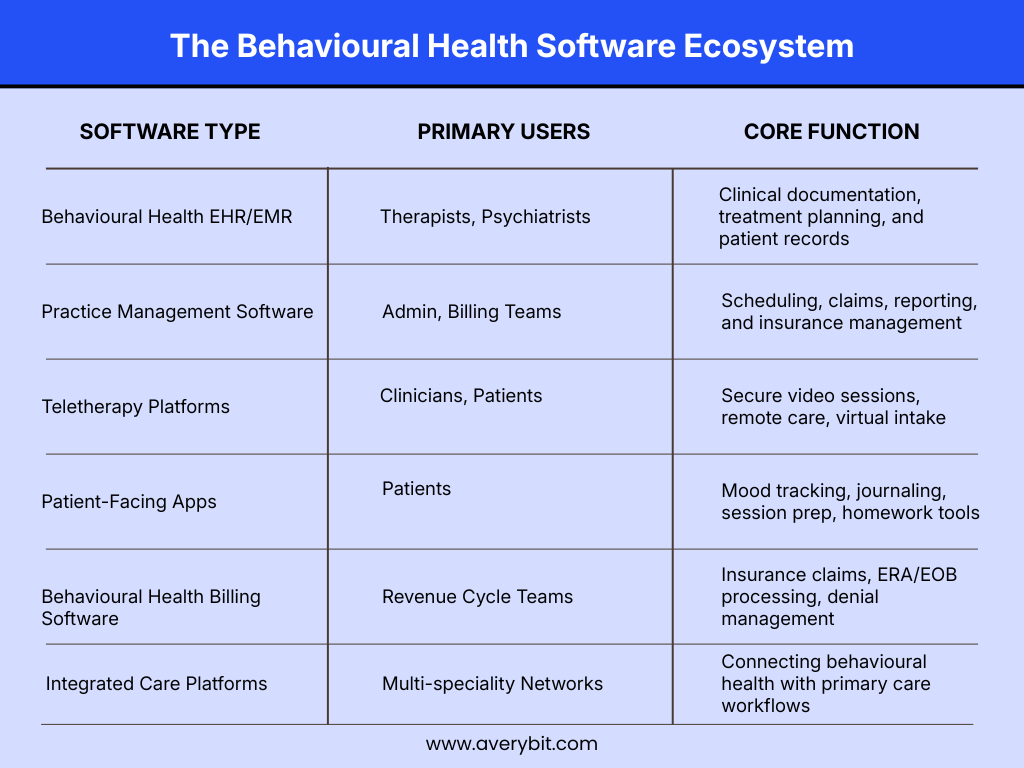
Behavioral health software is not simply a mental health app. It is a type of specialized software that has been designed for therapy clinics, psychiatric practices, substance use disorder treatment, and integrated care organizations. This type of software is used for clinical documentation, scheduling, billing, and compliance, and sometimes for patient engagement tools such as telehealth and progress tracking.
The reason you cannot simply use a general EHR solution for this is actually quite simple: the way that behavioral health care is practiced is different. Therapy sessions are very long and occur on a weekly basis for months or even years. The documentation is narrative, not simply checkbox-driven. Patient confidentiality regulations are more stringent. And if you are treating substance use disorders, you are working under a whole different level of federal regulatory compliance that general healthcare software solutions simply do not address.
The most common types of behavioral health software include EHR solutions designed specifically for therapy, practice management software designed for scheduling and billing, teletherapy software, patient engagement apps, and integrated care software that links behavioral health with primary care.
Should You Build It or Buy It?
This is often the first real decision organizations must make regarding their behavioral health operations; the answer is not necessarily the same for every solution:
Build custom if:
- Your organization uses a unique workflow that cannot be handled by off-the-shelf products.
- Your organization is scaling to more than one location and needs to ensure consistent operations across all locations.
- Your organization needs to maintain compliance with the federal regulations on the use of substance abuse records (42 CFR Part 2)
- The per-seat licensing cost is becoming a burden or is higher than the total cost of ownership of a custom build, estimated to exceed this cost.
Stick to off-the-shelf solutions if:
- You are a smaller firm with average-sized needs,
- You require quick results,
- You don’t have the budget nor the personnel to maintain ongoing software.
Consider a hybrid approach
Alternatively, consider a hybrid approach, using a configurable core platform with customized plugins on top of it, if you fall between off-the-shelf and fully custom solutions. This is particularly beneficial for mid-sized organizations.
Features That Actually Matter
Avoid the major pitfalls common to so many software development projects, in which teams attempt to create multiple features simultaneously, resulting in bloated products that no one wants, and ultimately delay launches by over 12 months, by focusing on only the core requirements for each type of user.
For Patients:
1) Ability to schedule appointments online easily
2) Ability to have secure video-based telehealth sessions with their providers
3) Punchline me in with a secure way to communicate with their provider without having to call the front desk
4) Simple tracking tools for their progress (PHQ-9, GAD-7, etc.) before each session using simple questionnaires
For Clinicians:
1) Templates that are built specifically for therapy, not just generic medical note templates (SOAP, DAP, BIRP)
2) Treatment plans that clearly connect to session notes to create high-quality, complete clinical trails
3) Group therapy documentation that does not require workarounds
4) e-Prescribing (if they are drug-permitting psychiatric providers)
Admin and operations teams need:
- Role-based user access so billing teams only see claims, but therapy notes are visible only to those who should see them.
- A billing module that accommodates behavioral health CPT Codes and captures insurance verifications.
- Audit logs indicating who accessed each record or document and when they accessed it
- Reports that do not require an IT person to run queries manually each time we need a report.
- AI-enhanced capabilities, population health dashboards, and advanced analytics should be included in phase 2 of your implementation. Count on having a good core product to begin with.
The Behavioral Health Software Development Process - A Realistic Roadmap
Realistically, the process of developing effective software in the realm of behavioral health is accomplished in phases; it incorporates active participatory involvement by real-life end-users early in development, includes validation of software compliance throughout all phases of development, and not just post-development.
Phase 1
Research. When you begin creating your new system, you need to speak with your actual users before you plan anything. Each group (Clinicians, admin, and billing) will have different areas of pain. If you look at the workarounds your users have devised in their current processes, you will begin to see where the real issues exist.
Phase 2
Determine the Minimum Viable Product (MVP). What is the smallest version of your system that is functional? Write that down! Secure approvals from all clinical, operational, and technical stakeholders. Once those approvals are secured, protect that scope – adding a feature post-approval will always cost more than expected.
Phase 3
Develop your Architecture Plan. Decide whether to build in the Cloud or On-premise, Monolithic or Microservices, and if you will build API First. Building API First is almost always the right decision because it will make any integrations you perform in the future much less costly.
Phase 4
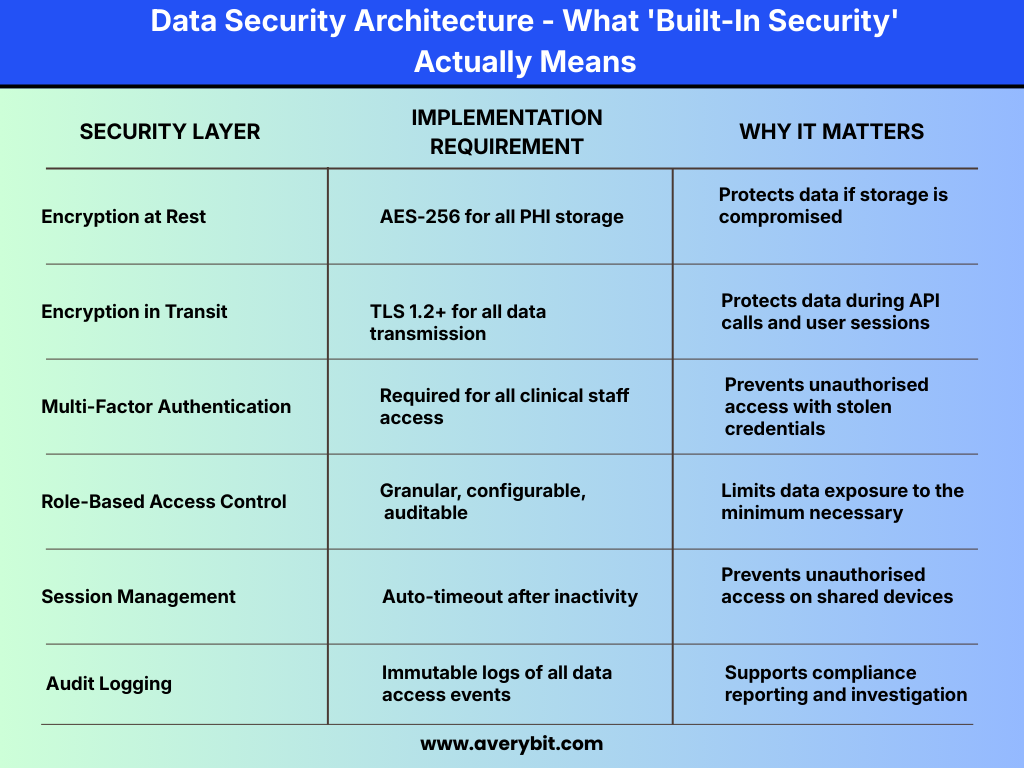
Build with Compliance Testing from Day 1. Do not wait till you are finished with your build to test security controls. Building Authentication, Access Control, and Audit Trails as part of your first sprint is the foundation for everything else you do in your build.
Phase 5
Data Migration. If you are replacing an existing system, this phase will take longer than you expect. You need to map your existing data fields to your new Field types, clean up any Data inconsistencies, validate that you transferred your data, and run both your new and old systems in Parallel for an agreeable time frame before cutting over completely to your new system.
Phase 6
This is the final phase of the project. After determining the best path forward during Phase 5 (testing), you should allow your organization time to implement the earning potential of these recommendations through a pilot involving only a few clinics or teams (generally lasting 4 to 6 weeks). Items learned during Phase 6 will need to be corrected before the rollout pace increases significantly. In addition to the pilot phase, establishing a budget for the long-term maintenance, security, and enhancements of your solution must occur. Generally, you should budget approximately 15–20% of your initial setup cost each year for these costs.
Analyzing Your Project's Failures
The above issues are not uncommon; in fact, they represent the issues that consistently cause failure or slow the success of projects that were otherwise set for success by the project team.
Delaying compliance.
You cannot add encryption, access controls, and auditing to a system that was not designed with these features as part of the original scope of the project; these compliance features must be a part of your project from inception.
2. Attempting to build everything in a single version of the product.
The issue of scope creep in most behavioral health software development projects is not the result of a single decision involving additional features. Rather, it is the hundreds of smaller “while we are here” additions that cumulatively exhaust the budget and timeline for the project. Successfully launch a useful solution; enhance it with future versions.
3. Hiring a software development firm without healthcare experience.
The majority of the time needed for a software-specific development firm is to get them up to speed on what they are doing. As a result, the cost to get them on board is a cost to your budget and timetable due to their lack of knowledge of the healthcare industry.
4. EHR Integrations Are a Bigger Deal than You Think
When connecting with a vendor like Epic Systems or Cerner Corporation, it’s not merely a technical job but rather a lengthy process that requires you to go through an official partnership with that vendor before any development work can start (typically going through a lengthy vendor process).
Don’t wait until the end of your project to consider how your software will interface with them; plan!
5. Not testing with real clinicians.
Operation of Your Software by Clinicians is Very Different than How Internal Staff Used Your Software
Your internal Quality Assurance process does not cover what will happen when your software is operated by a licensed therapist for the very first time. Your best approach is to get clinicians involved early on – from the wireframe stage.
6. You Must Consider the 42 CFR Part 2 Assessment Before Developing Your Data Architecture
If you serve clients who are in recovery from substance use disorders, you should conduct an assessment of your ability to comply with 42 CFR Part 2 before developing your final data architecture. Finding out after you developed your system that you are not in compliance can quickly become an expensive problem.
What's Coming Next in Behavioral Health Software
The way behavioral health is reimbursed is being transformed by value-based care. Platforms that track and report on patient outcomes – not just the number of sessions – will have the upper hand as payer contracts change. One example of this is the growth of asynchronous therapy, text-only non-live therapy, which has been shown through clinical evidence to benefit specific populations or clinical presentations. However, if your platform only offers video therapy sessions, you will be missing out on an entire segment of the market.
As FHIR interoperability continues to become an expectation of healthcare networks, providers of behavioral health technology can no longer expect to operate without the ability for bidirectional exchange of data. You will lose the contract if you do not have a connection.
Choosing the Right Development Partner
More than almost anything else, this decision will impact your project.
When evaluating healthcare software development organizations with which to partner, look for those that have experience building solutions in this space and can demonstrate their past projects (case studies with quantitative outcome data). Ensure they can describe an example of how they have delivered a solution using a specific FHIR Integration project. As a final check, ask them what 42 CFR Part 2 stipulates, without giving them a definition.
Be suspicious of vendors that promote compliance as simple and are registered with many consumer applications in their portfolio (but no health care clients) and do not want to follow a staged development strategy.
A good vendor will have in-depth industry experience so that they do not require you to explain the fundamentals of the business to them.
Abschließende Gedanken
Correctly developed behavioral health software optimizes clinical workflows through reduced documentation, increased patient interaction time, and improved clinical outcomes.
The primary differentiators between systems that produce good results or poor results will be based on comprehensive project planning, discipline related to delivery timelines, and the best vendor association for software development.
At AveryBit, we develop healthcare-related software solutions that clinical users want to work with; if you would like more information regarding where to start your project, please contact us.